Causes of a Peripheral Neuropathy :
Predominantly sensory
Common causes include :
Diabetes mellitus
Alcohol
Drugs – eg isoniazid and vincristine
Vitamin deficiency eg B1 and B 12
Predominantly motor :
Guillain Barre Syndrome and Botulism – present acutely
Lead toxicity
Porphyria
HSMN : Hereditary Sensori Motor Neuropathy
Mononeuritis Multiplex
Diabetes
Connective Tissue Disease eg SLE and Rheumatoid arthritis
Vasculitis eg PAN : Polyarteritis Nodosa and CSS Churg Strauss Syndrome
Infection eg HIV
Malignancy
Thursday, 16 April 2020
History Taking : Chest Pain
History taking Scenario
Your Role :
You are the medical SHO /RMO on call clerking in A & E and are asked to assess a young man with chest pain.
Your patient : T L , age 21
This young man presents with chest pain.He has been out clubbing with his friends on Saturday night and developed sudden onset of retrosternal chest pain radiating to the back with associated shortness of breath.
His father suffered from an MI at age of 50 years.
He is concerned that he is having an MI.
His Chest X ray shows a pleural effusion on right side.
The ECG shows a Sinus Tachycardia but is otherwise un remarkable.
Blood Tests are awaited.
Please take a detailed history from this patient keeping in mind the major differential diagnoses.
Main points and approach to the scenario:
Greet the examiners
Read the scenario carefully with focus on patients name ,age and presenting complaint.
Assess/ determine what is being asked from you in the scenario.
Take time to read the scenario fully in the required time frame.
Asssess the time you have to complete a focused and clear history and make sure you rule out the main alarming conditions first that present with chest pain.
For example in this scenario , Set Your objectives
You have to take a focused and comprehensive History to exclude the conditions below :
Differential Diagnosis:
Esophageal Rupture
Pulmonary Embolism
Aortic Dissection
Acute Myocardial Infarction
GORD : Gastroesophageal reflux disease
Acute Pancreatitis
Pneumothorax
Now Greet the patient and Introduce Yourself
History Of Present Illness
Take a detailed account of history of present illness following the format:
ODPARRA:
Onset
Duration
Progression
Associated Factors
Relieving Factors
Radiation
Aggravating Factors
Here is how to begin this station
Good Morning Mr L
My name is Dr AR and I am here to ask you a few questions to better understand the casue of your coming to the hospital today
Is it alright if I proceed?
Are you feeling comfortable ?
The above questions are important to ask as they constitute an important score in exam which is called Maintaining Patients Welfare.
So can you please tell me in your own words what brought you to hospital today ?
Listen carefully to what patients says noting any new points that were not present in patients history.
Onset :
Can you please tell how did the problems start?
Was it sudden in onset or have you been feeling it for some time and it got accentuated?
Duration:
How long this stay for.
Over what period of time did this happen.
If repetitive problem ,how long has this been happening ?
Is it constant or intermittent ?
Progression:
Did it get worse? Stayed the same ? or improved ?
Associated Factors :
Any nausea ,sweating , fever , vomiting ,sob : Cardiac
PND , orthopnea ,ankle oedema : Left ventricular failure.
Abdominal pain ?
Any trauma to chest etc
Any cough haemoptysis : PE and LRTI
Any unilateral swelling of leg DVT.
Any recent history of travel abroad ?
Cold/flu like symptoms : Pericarditis
Excessive drinking before the episode : Esophageal perforation
Radiation:
Any radiation of the pain somewhere eg back etc,
Aortic dissection, pancreatitis and peptic ulcer radiate to the back.
Cardiac ischaemic pain radiates to left jaw,neck and left arm.
Nerve root pain remains around the chest wall in a band like pattern.
Relieving factors :
Any thing that made it better eg medication , change in position etc
Analgesics : Musculoskeletal pain
Cardiac pain : rest and nitrates.
Antacids : GORD and PUD.
Aggravating Factors :
Any thing that made it worse?
Deep inspiration : pericarditis and respiratory.
Movement : Musculoskeletal.
Eating / after meals : peptic ulcer disease and GORD.
Bending forward : pericarditis.
Exertion ? Cardiac.
Family History of IHD , Hypercholesterolemia , Angina , Asthma ,MI , Hypertension , Epilepsy or bleeding disorders
Site of chest pain”
Cardiac : central and often radiates to left jaw neck and left arm.Is brought with exertion and may be associated with shortness of breath.
Respiratory : is usually present on site of pathology eg infection or pneumothorax.
Musculoskeletal : is present at site of pathology or injury
Peptic ulcer disease / GORD occurs in lower chest and epigastrium.
Nature of pain :
Cardiac / ischemic : Dull pressure like sensation.
Pericarditis and Respiratory : sharp and pleuritic.
Nerve root pain : band like shooting pain around the chest from the back to the front.
GORD : sharp and burning
Personal History
Any habitual smoking or drinking alcohol ?
Past Medical and Family history :
Cardiovascular risk factors :
Smoking , hypertension,diabetes,hypercholesterolemia and family history of these.
Any compliance to treatment
Previous MI or CABG / BYPASS etc
History of clotting / thrombotic disorders
Medications and their compliance
Occupational history
Assess the disability and impact on life
Address the patients concerns about this
Plan of Management :
Tell the patient the most likely Differental Diagnosis and other possible causes
In this case this seems like an Esophageal perforation but other D/D are:
Pulmonary Embolism
Aortic Dissection
Acute Myocardial Infarction
GORD : Gastroesophageal reflux disease
Acute Pancreatitis
Pneumothorax
Pleurisy
Pneumonia
Pericarditis
Further investigations will be needed to ascertain the cause eg
Chest X ray
ECG
Oxyge saturations
Full Blood Count
D- dimers
Arterial Blood gases
CTPA
Your Role :
You are the medical SHO /RMO on call clerking in A & E and are asked to assess a young man with chest pain.
Your patient : T L , age 21
This young man presents with chest pain.He has been out clubbing with his friends on Saturday night and developed sudden onset of retrosternal chest pain radiating to the back with associated shortness of breath.
His father suffered from an MI at age of 50 years.
He is concerned that he is having an MI.
His Chest X ray shows a pleural effusion on right side.
The ECG shows a Sinus Tachycardia but is otherwise un remarkable.
Blood Tests are awaited.
Please take a detailed history from this patient keeping in mind the major differential diagnoses.
Main points and approach to the scenario:
Greet the examiners
Read the scenario carefully with focus on patients name ,age and presenting complaint.
Assess/ determine what is being asked from you in the scenario.
Take time to read the scenario fully in the required time frame.
Asssess the time you have to complete a focused and clear history and make sure you rule out the main alarming conditions first that present with chest pain.
For example in this scenario , Set Your objectives
You have to take a focused and comprehensive History to exclude the conditions below :
Differential Diagnosis:
Esophageal Rupture
Pulmonary Embolism
Aortic Dissection
Acute Myocardial Infarction
GORD : Gastroesophageal reflux disease
Acute Pancreatitis
Pneumothorax
Now Greet the patient and Introduce Yourself
History Of Present Illness
Take a detailed account of history of present illness following the format:
ODPARRA:
Onset
Duration
Progression
Associated Factors
Relieving Factors
Radiation
Aggravating Factors
Here is how to begin this station
Good Morning Mr L
My name is Dr AR and I am here to ask you a few questions to better understand the casue of your coming to the hospital today
Is it alright if I proceed?
Are you feeling comfortable ?
The above questions are important to ask as they constitute an important score in exam which is called Maintaining Patients Welfare.
So can you please tell me in your own words what brought you to hospital today ?
Listen carefully to what patients says noting any new points that were not present in patients history.
Onset :
Can you please tell how did the problems start?
Was it sudden in onset or have you been feeling it for some time and it got accentuated?
Duration:
How long this stay for.
Over what period of time did this happen.
If repetitive problem ,how long has this been happening ?
Is it constant or intermittent ?
Progression:
Did it get worse? Stayed the same ? or improved ?
Associated Factors :
Any nausea ,sweating , fever , vomiting ,sob : Cardiac
PND , orthopnea ,ankle oedema : Left ventricular failure.
Abdominal pain ?
Any trauma to chest etc
Any cough haemoptysis : PE and LRTI
Any unilateral swelling of leg DVT.
Any recent history of travel abroad ?
Cold/flu like symptoms : Pericarditis
Excessive drinking before the episode : Esophageal perforation
Radiation:
Any radiation of the pain somewhere eg back etc,
Aortic dissection, pancreatitis and peptic ulcer radiate to the back.
Cardiac ischaemic pain radiates to left jaw,neck and left arm.
Nerve root pain remains around the chest wall in a band like pattern.
Relieving factors :
Any thing that made it better eg medication , change in position etc
Analgesics : Musculoskeletal pain
Cardiac pain : rest and nitrates.
Antacids : GORD and PUD.
Aggravating Factors :
Any thing that made it worse?
Deep inspiration : pericarditis and respiratory.
Movement : Musculoskeletal.
Eating / after meals : peptic ulcer disease and GORD.
Bending forward : pericarditis.
Exertion ? Cardiac.
Family History of IHD , Hypercholesterolemia , Angina , Asthma ,MI , Hypertension , Epilepsy or bleeding disorders
Site of chest pain”
Cardiac : central and often radiates to left jaw neck and left arm.Is brought with exertion and may be associated with shortness of breath.
Respiratory : is usually present on site of pathology eg infection or pneumothorax.
Musculoskeletal : is present at site of pathology or injury
Peptic ulcer disease / GORD occurs in lower chest and epigastrium.
Nature of pain :
Cardiac / ischemic : Dull pressure like sensation.
Pericarditis and Respiratory : sharp and pleuritic.
Nerve root pain : band like shooting pain around the chest from the back to the front.
GORD : sharp and burning
Personal History
Any habitual smoking or drinking alcohol ?
Past Medical and Family history :
Cardiovascular risk factors :
Smoking , hypertension,diabetes,hypercholesterolemia and family history of these.
Any compliance to treatment
Previous MI or CABG / BYPASS etc
History of clotting / thrombotic disorders
Medications and their compliance
Occupational history
Assess the disability and impact on life
Address the patients concerns about this
Plan of Management :
Tell the patient the most likely Differental Diagnosis and other possible causes
In this case this seems like an Esophageal perforation but other D/D are:
Pulmonary Embolism
Aortic Dissection
Acute Myocardial Infarction
GORD : Gastroesophageal reflux disease
Acute Pancreatitis
Pneumothorax
Pleurisy
Pneumonia
Pericarditis
Further investigations will be needed to ascertain the cause eg
Chest X ray
ECG
Oxyge saturations
Full Blood Count
D- dimers
Arterial Blood gases
CTPA
Saturday, 11 April 2020
Communication Skills : Breaking Bad News Scenario
Mr J is a 68 years old male who has been having increasing shortness of breath,back ache and swelling of both feet since last 4 months.
He has been investigated now and it is found out he has Metastatic Renal Carcinoma and after discussion with oncologist ,he says it is not possible to treat it by Surgery and only symptomatic / Supportive Rx can be given.
He is also found to have Congestive Cardiac Failure . Oncologist thinks he has only 4 months to live.
Break this Bad News to him.
Key points :
Introduce your self and confirm identity of patient.
Establish purpose of meeting and also ask the patient what he knows about his condition,blood and imaging tests and other investigations.
Try to establish if he knows what the problem might be ?
“ Do you know the purpose of our meeting today ? “
“ What do you think is wrong with you ?”
“We did some tests and the results are back” .
“I am afraid the results are not too good “
“ Do you want me to proceed with the results? “
“ Do you want to know the results of these investigations ?
“ Do you want me to call someone from your home to accompany you ?
“ You have been diagnosed with cancer of the Right kidney.
Offer some time for the patient to take this news before proceeding further.
Offer patients some tissues if possible.
Ask if he wants us to proceed further with more findings,if he wishes so ,tell him about his Metastasis finding .
“I am afraid the cancer has spread to other parts of your body from your kidney and the oncologist does not believe treatment of this cancer at this stage can be done ,neither surgery nor chemotherapy as it has widespread “.
But we will give you treatment for pain control and nausea .
Patient asks how much time do I have ?
Tell him ,the oncologist says you have only 4 more months to live.
Be specific and clear and honest about predicted prognosis.
Patient said he wants to go on holiday.
Encourage him to enjoy his time by going to holiday and doing the things and hobbies he likes to do and encourage him to spend time with his family as well.
Ask about his hobbies and tell him to engage in them.
Also if he wants to have another meeting with his family present .
Tell him to avoid dangerous hobbies but can have safe one
He has been investigated now and it is found out he has Metastatic Renal Carcinoma and after discussion with oncologist ,he says it is not possible to treat it by Surgery and only symptomatic / Supportive Rx can be given.
He is also found to have Congestive Cardiac Failure . Oncologist thinks he has only 4 months to live.
Break this Bad News to him.
Key points :
Introduce your self and confirm identity of patient.
Establish purpose of meeting and also ask the patient what he knows about his condition,blood and imaging tests and other investigations.
Try to establish if he knows what the problem might be ?
“ Do you know the purpose of our meeting today ? “
“ What do you think is wrong with you ?”
“We did some tests and the results are back” .
“I am afraid the results are not too good “
“ Do you want me to proceed with the results? “
“ Do you want to know the results of these investigations ?
“ Do you want me to call someone from your home to accompany you ?
“ You have been diagnosed with cancer of the Right kidney.
Offer some time for the patient to take this news before proceeding further.
Offer patients some tissues if possible.
Ask if he wants us to proceed further with more findings,if he wishes so ,tell him about his Metastasis finding .
“I am afraid the cancer has spread to other parts of your body from your kidney and the oncologist does not believe treatment of this cancer at this stage can be done ,neither surgery nor chemotherapy as it has widespread “.
But we will give you treatment for pain control and nausea .
Patient asks how much time do I have ?
Tell him ,the oncologist says you have only 4 more months to live.
Be specific and clear and honest about predicted prognosis.
Patient said he wants to go on holiday.
Encourage him to enjoy his time by going to holiday and doing the things and hobbies he likes to do and encourage him to spend time with his family as well.
Ask about his hobbies and tell him to engage in them.
Also if he wants to have another meeting with his family present .
Tell him to avoid dangerous hobbies but can have safe one
Tuesday, 7 April 2020
Nervous System Examination Routine
NERVOUS SYSTEM EXAMINATION
Mr K is a 58 years old gentleman who has been having difficulty in walking.
Please examine the Neurological system and lower limbs of this patient.
How to approach the case
Greet the patient and introduce yourself.
Steps in Examination :
Aim to shake his hand.Once a candidate had a patient with Myotonic dystrophy in one of the exams.
When he shook his hand , he wouldn’t let go. He had myotonic dystrophy which the candidate failed to pick due to examination anxiety.
Tell him I am Dr S and I want to examine your legs.
If you are comfortable ,is it OK if I proceed with the examination?
Look at the face of the patient . Any particular facies ? ( e g mask like face )
Any Ptosis ?/ Droping of eyelid?
Any obvious cranial nerve palsy eg eye deviated out and down etc ?
Look at the back for Scoliosis , Scar marks , Winging of scapula etc ?
Look at the legs of the patient for any wasting , fasciculations , abnormal movements etc.
Gait :
Now ask the patient to get up and take a few steps forward to the wall and have a look at his gait.
At this point it would be great idea to walk close to the patient , supporting him in the event if he falls at all.
Now tell the patient to walk back aiming to test Tandem walking .
(Tandem gait is a gait where the toes of the back foot touch the heel of the front foot at each step. Neurologists sometimes ask patients to walk in a straight line using tandem gait as a test to help diagnose ataxia, especially truncal ataxia, because sufferers of these disorders will have an unsteady gait.)
Tell patient to stand up straight and close his eyes and support him. ( Romberg”s Test)
The Romberg test is used to investigate the cause of loss of motor coordination (ataxia). A positive Romberg test suggests that the ataxia is sensory in nature, that is, depending on loss of proprioception. If a patient is ataxic and Romberg's test is not positive, it suggests that ataxia is cerebellar in nature, that is, depending on localized cerebellar dysfunction instead.
Tell the patient to walk back into the bed,supporting him
Tone
Now examine tone of the legs
Check for ankle clonus and plantars as well.
Power / Motor Examination
Examine the power of lower legs.
Sensory Examination
Now do a quick sensory examination and reflexes of the lower limbs including ankle and knee jerk.
Reflexes:
Plantars
Co-ordination
Examine co-ordination of the legs including heel knee shin test.
Cerebellar signs
Look for cerebellar signs including intention tremor and Disdiadochokinesis.
In sensory system examination,look for Pin prick,temperature ,joint position and two point discrimination.
If possible,do a fundoscopy / atleast mention it.
Aim to see if patient has a drug chart and taking any medications.
Diagnosis of the patient :
The patient had Ataxic gait .This is seen in patient having lesions of the central part of the cerebellum
Positive Romberg.
Romberg's test is positive in conditions causing sensory ataxia such as:
Vitamin deficiencies such as Vitamin B12
Conditions affecting the dorsal columns of the spinal cord, such as tabes dorsalis (neurosyphilis), in which it was first described.
Conditions affecting the sensory nerves (sensory peripheral neuropathies), such as chronic inflammatory demyelinating polyradiculoneuropathy (CIDP).
Friedreich's ataxia
Ménière's disease
Mr K is a 58 years old gentleman who has been having difficulty in walking.
Please examine the Neurological system and lower limbs of this patient.
How to approach the case
Greet the patient and introduce yourself.
Steps in Examination :
Aim to shake his hand.Once a candidate had a patient with Myotonic dystrophy in one of the exams.
When he shook his hand , he wouldn’t let go. He had myotonic dystrophy which the candidate failed to pick due to examination anxiety.
Tell him I am Dr S and I want to examine your legs.
If you are comfortable ,is it OK if I proceed with the examination?
Look at the face of the patient . Any particular facies ? ( e g mask like face )
Any Ptosis ?/ Droping of eyelid?
Any obvious cranial nerve palsy eg eye deviated out and down etc ?
Look at the back for Scoliosis , Scar marks , Winging of scapula etc ?
Look at the legs of the patient for any wasting , fasciculations , abnormal movements etc.
Gait :
Now ask the patient to get up and take a few steps forward to the wall and have a look at his gait.
At this point it would be great idea to walk close to the patient , supporting him in the event if he falls at all.
Now tell the patient to walk back aiming to test Tandem walking .
(Tandem gait is a gait where the toes of the back foot touch the heel of the front foot at each step. Neurologists sometimes ask patients to walk in a straight line using tandem gait as a test to help diagnose ataxia, especially truncal ataxia, because sufferers of these disorders will have an unsteady gait.)
Tell patient to stand up straight and close his eyes and support him. ( Romberg”s Test)
The Romberg test is used to investigate the cause of loss of motor coordination (ataxia). A positive Romberg test suggests that the ataxia is sensory in nature, that is, depending on loss of proprioception. If a patient is ataxic and Romberg's test is not positive, it suggests that ataxia is cerebellar in nature, that is, depending on localized cerebellar dysfunction instead.
Tell the patient to walk back into the bed,supporting him
Tone
Now examine tone of the legs
Check for ankle clonus and plantars as well.
Power / Motor Examination
Examine the power of lower legs.
Sensory Examination
Now do a quick sensory examination and reflexes of the lower limbs including ankle and knee jerk.
Reflexes:
Plantars
Co-ordination
Examine co-ordination of the legs including heel knee shin test.
Cerebellar signs
Look for cerebellar signs including intention tremor and Disdiadochokinesis.
In sensory system examination,look for Pin prick,temperature ,joint position and two point discrimination.
If possible,do a fundoscopy / atleast mention it.
Aim to see if patient has a drug chart and taking any medications.
Diagnosis of the patient :
The patient had Ataxic gait .This is seen in patient having lesions of the central part of the cerebellum
Positive Romberg.
Romberg's test is positive in conditions causing sensory ataxia such as:
Vitamin deficiencies such as Vitamin B12
Conditions affecting the dorsal columns of the spinal cord, such as tabes dorsalis (neurosyphilis), in which it was first described.
Conditions affecting the sensory nerves (sensory peripheral neuropathies), such as chronic inflammatory demyelinating polyradiculoneuropathy (CIDP).
Friedreich's ataxia
Ménière's disease
Sunday, 5 April 2020
History Taking : Shortness of Breath
Introduction
My name is Dr A and I am here today to ask you a few questions about what brings you to hospital today.
I believe you have been having increasing shortness of breath.
Would you be able to tell me in more detail about it so we can try to find out t he possible causes for this.
History of present Illness
ODPARRA
Onset :
Can you please tell me how did the problem start?
Did it happen suddenly or over a period of time ?
Establish a baseline functional status : What was your breathing like about 6 months ago ?
Is the breathlessness constant or intermittent ?
If intermittent , how frequently do you experience breathlessness ?
Duration:
How long has this been going on for?
Is it the first time you have experienced this or has it happened before?
Progression:
Is it getting worse with time ? or staying same or improving ?
Aggravating Factors :
What worsens your shortness of breathlesness.
Is it present at rest ?
Does exertion make it worse ?
Does it get worse on lying down ?
Relieving Factors :
Does it get better with rest ?
Do any medications make it better ? eg nebulizers,inhalers or sub lingual nitrates ?
Associated Factors
Any chest pain ?
This is suggestive of ischemic / cardiac origin.
Any palpitations :
They indicate presence of underlying arrhythmia which can be exertional and would mean : AF / atrial flutter or ventricular arrhythmias.
Ask the patient is their heart beat regular or irregular during arrhythmia and if they could tap out the beat.
Also if they have measured their heart beat.
Any Orthopnea or PND: Paroxysmal Nocturnal Dyspnea are suggested of left Ventricular Dysfunction.
Peripheral oedema is suggestive of CCF or Cor – pulmonale.
Respiratory symptoms :
Any cough ? Dry or productive,
Any wheeze , Any Haemoptysis ?
If productive color of sputum and amount
A dry non- productive cough suggests viral etiology,or Interstitial lung disease
A productive / suppurative cough is suggestive of infection,suppurative lung diseases or malignancy.
Haemoptysis occurs in malignancy , PE or infection or pulmonary congestion especially with mitral stenosis
Any exceesive use of steroids ( eg Asthma or Rheumatoid arthritis causing immunusupression leading to PCP pneumonia )
Vasculitic symptoms and Sarcoidosis
Any leg pains
Any skin rash
Muscle aches suggestive of vasculitis
Any increased use of steroids ( can cause pneumocystis carinii pneumonia )
Any History of HIV / Immunosuppression ( can cause pneumocystis carinii pneumonia )
Any cold , fevers : Any flu like symptoms :Viral etiology
Any weight loss : Malignancy / TB
Do you keep any pets : Psittacosis / allergic bronchitis
What is your occupation : Occupational lung disease : Do symptoms improve when away from work ?
Any irritation in eyes
Any swollen glands ? ( lymphadenopathy) : TB / Sarcoidosis / Malignancy
Any recent contact with some one with TB
Any change in bowel habits
Any blood in stools
Ay Jaundice ( Yellow discoloration of eyes/ sclera)
Any recent travel abroad
Any use of Recreational drugs : or IV abuse ( HIV / Hepatitis B / Immunosuppression )
Medications :
Ask about full list of medications and compliance to therapy.
Appetite suppressors eg fenfluramine is associated with pulmonary hypertension.
Social Issues :
Ask about smoking ( cigarettes / day and pack years)
Alcohol consumption
Occupation
Impact of symptoms on daily living.
Any concerns the patient may be having ?
Saturday, 21 March 2020
Corona outbreak : Steps to prevent further spread of virus
https://www.medstudentnotes.com/?ref=SAADSHAH
Corona pandemic is out these days and it has caused mortalities in many countries.
Most fatalities have occured in China,Italy,Spain,Germany,Iran,France,UK , USA,Canada,Switzerland,Iraq,Turkey,Netherlands and Japan and our condolences goes to all of their families who have lost their loved ones.
Like all other viruses,it affects people of different age groups variably depending on their age and existing health and symptoms are ranging from mild cough,flu like symptoms in healthy and young people but it has more severe manifestations on elderly people with pre-existing health problems.
While research is on going to devise vaccinations and devise treatment for this disease,in the meantime,full focus should be to prevent spread of this diseases and keep those who have contracted this bug to keep them under treatment in isolation but ensuring their full support both psychologically and physically.
Also for those who have full support and resources available,it would be very good gesture to help support your neighbours or people who are less lucky and provide them or share with them some of your resources if you have surplus amount of them as it is community at large which is at risk and less the people exposed to risk,the more beneficial for over all health of the community.
Here are some steps we can take to keep ourselves protected from further spreading this virus :
1. Eat healthy ,ensuring intake of plenty of fruits ,vegetables and water and keep your self well hydrated.
2. Avoid going to crowded places and wear mask to cover your mouth and nose if inevitable such as going out for shopping .
3.Avoid un-necessary functions and gatherings such as birthday parties.
4.Avoid handshaking , un necessary contact and avoid sharing utensils,towels etc.
5. Keep frequent hand washing with soap for at least 20 seconds and use hand sanitizers after any outside visit or touching any surfaces .
6.Cover your mouth and nose while coughing / sneezing.
7.If you have flu like symptoms,try to keep yourself isolated for at least 2 weeks and keep a safe distance from others.
8.Avoid ice creams/cold drinks or other foods that can cause you to develop sorethroat/pharyngitis.
https://www.medstudentnotes.com/?ref=SAADSHAH
Further guidance is available in links below :
https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public
https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-prevent-spread.html
Hoping for health and well being and safety of everyone.
Corona pandemic is out these days and it has caused mortalities in many countries.
Most fatalities have occured in China,Italy,Spain,Germany,Iran,France,UK , USA,Canada,Switzerland,Iraq,Turkey,Netherlands and Japan and our condolences goes to all of their families who have lost their loved ones.
Like all other viruses,it affects people of different age groups variably depending on their age and existing health and symptoms are ranging from mild cough,flu like symptoms in healthy and young people but it has more severe manifestations on elderly people with pre-existing health problems.
While research is on going to devise vaccinations and devise treatment for this disease,in the meantime,full focus should be to prevent spread of this diseases and keep those who have contracted this bug to keep them under treatment in isolation but ensuring their full support both psychologically and physically.
Also for those who have full support and resources available,it would be very good gesture to help support your neighbours or people who are less lucky and provide them or share with them some of your resources if you have surplus amount of them as it is community at large which is at risk and less the people exposed to risk,the more beneficial for over all health of the community.
Here are some steps we can take to keep ourselves protected from further spreading this virus :
1. Eat healthy ,ensuring intake of plenty of fruits ,vegetables and water and keep your self well hydrated.
2. Avoid going to crowded places and wear mask to cover your mouth and nose if inevitable such as going out for shopping .
3.Avoid un-necessary functions and gatherings such as birthday parties.
4.Avoid handshaking , un necessary contact and avoid sharing utensils,towels etc.
5. Keep frequent hand washing with soap for at least 20 seconds and use hand sanitizers after any outside visit or touching any surfaces .
6.Cover your mouth and nose while coughing / sneezing.
7.If you have flu like symptoms,try to keep yourself isolated for at least 2 weeks and keep a safe distance from others.
8.Avoid ice creams/cold drinks or other foods that can cause you to develop sorethroat/pharyngitis.
https://www.medstudentnotes.com/?ref=SAADSHAH
Further guidance is available in links below :
https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public
https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-prevent-spread.html
Hoping for health and well being and safety of everyone.
Tuesday, 11 February 2020
Pharmacology Made Simple : Rifaximin
Mechanism Of Action.
Rifaximin is a semi-synthetic derivative of rifampin and acts by binding to the beta-subunit of bacterial DNA-dependent RNA polymerase blocking one of the steps in transcription.
This results in inhibition of bacterial protein synthesis and consequently inhibits the growth of bacteria.
Chemical Structure Of Rifaximin

Uses Of Rifaximin

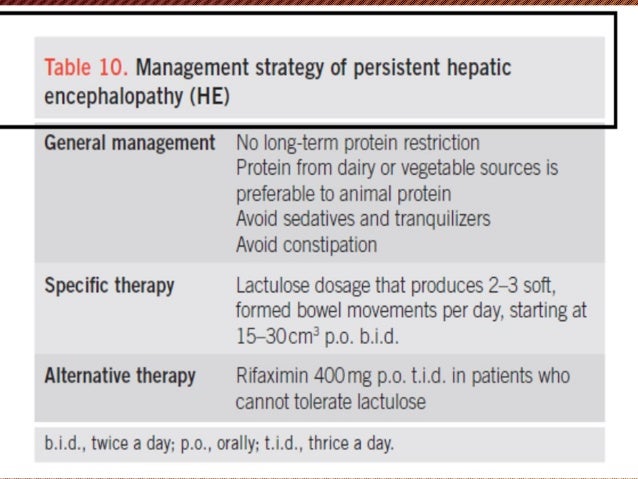
Rifaximin Use in Hepatic Encephalopathy:

Other uses include treatment of: infectious diarrhea, small intestinal bacterial overgrowth, inflammatory bowel disease, and diverticular disease.
Rifaximin is effective in treating small intestinal bacterial overgrowth regardless of whether it is associated with irritable bowel syndrome or not.
BASIC STEPS IN MANAGEMENT OF HEPATIC ENCEPHALOPATHY

Subscribe to:
Posts (Atom)