Steps involved in Emergency Treatmemt of Eye Injuries

https://go.urtrackinglink.com/aff_c?offer_id=1342&aff_id=24051


https://go.urtrackinglink.com/aff_c?offer_id=1342&aff_id=24051
A 45 year old man presents to your clinic with complaints of increasing shortness of breath over last 6 months.
He also gets occasional episodes of dry cough when walking or going up stairs.
On examination :
He is afebrile / normal Temperature and oxygen saturation is 89 Percent on air .
You organise a chest X ray which is given below:
1. What are findings on chest X ray?
2. What is the most likely Diagnosis?
3. What are the causes of this condition?
4. What further investigations would you like to perform?
5. How would you manage this condition?
Copyright reserved with author.
Answers given in comments section.
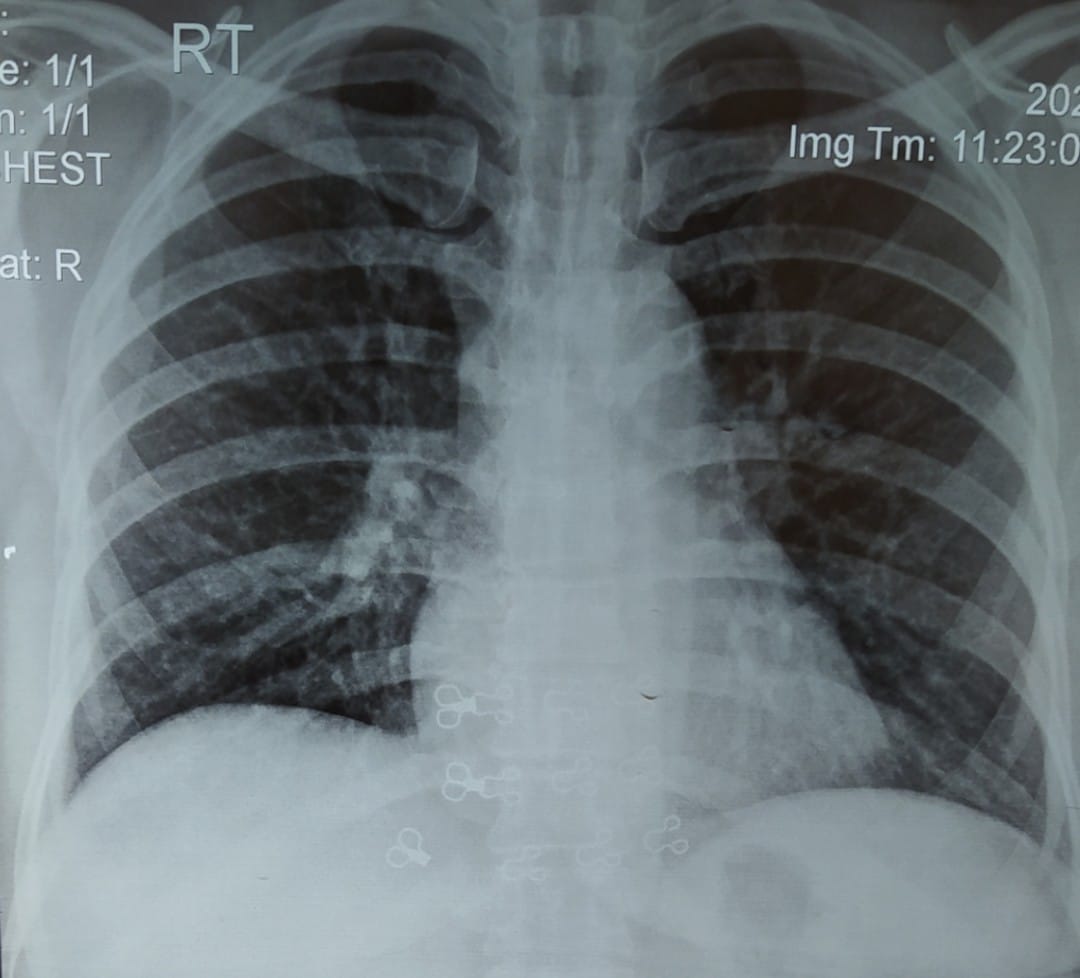
2. What is the most likely Diagnosis?
Interstitial Lung Disease (ILD) Interstitial Lung Disease (ILD) refers to a group of problems in the lung that affects the “interstitium”.
The interstitium refers to the tissue area in and around the wall of the airsacs (alveoli) of the lung area where oxygen moves from the alveoli into the the capillary network (small blood vessels) that covers the lung like a thin sheet of blood.
Once the oxygen crosses the intersitial space it enters the bloodstream and is delivered to the vital organs of your body. ILDs cause this interstitial space to become inflammed or scarred making it more difficult for oxygen.
3. What are the causes of this condition ? Causes of ILD
There are many causes of ILDs and they can be categorized as pictured above into three broad, main groups:
1) Exposure-Related,
2) Autoimmune-Related and
3) Idiopathic, or with no known cause. Exposure-Related (Hypersensitivity Pneumonitis or 'HP'):
Inhalation-related:
There are more than 300 causes of inhalational exposure-related ILDs.
These exposures can be experienced in the workplace, at home, while doing hobbies, or during travel.
Some of the more common exposures are mold, birds in or around the home, bedroom, or backyard, farming/agricultural work, indoor hot tubs, standing water, down feathers, and cleaning chemicals.
Historically, coal miners (pneumoconiosis) and exposure to asbestos (asbestosis) were significant problems, but these exposures have lessened due to the use of protective respiratory equipment.
Medication-related: Some of the medications that can cause an inflammatory reaction in the lung include amiodarone, methotrexate, some chemotherapy agents used to treat cancers, and nitrofurantoin (sulfa drugs).
Autoimmune-Related ILDs (Nonspecific Interstitial Pneumonitis – NSIP): Autoimmune–related ILDs tend to occur more often in women and in persons under the age of 65. Idiopathic ILDs (no known cause):
Idiopathic Pulmonary Fibrosis (IPF) is the most common ILD that has no known cause.
4. What further investigations would you like to perform? Radiology evaluations:
A Computed Tomography (CT) scan of the chest is the most sensitive diagnostic tool for ILD. The best assessment is with a high resolution CT scan (HRCT) which provides thin slices (1-2 mm thick) of the lungs in order to closely evaluate the lung tissue changes. Chest X-Rays may show ILD but are not diagnostic. Breathing tests:
Pulmonary Function Studies (PFTs) are used to evaluate the severity of the lung problem. PFTs evaluate the ability of the lung to:
move air in and out of the lungs (spirometry- Forced Vital Capacity (FVC), Forced Expiratory Volume in 1 second (FEV1). Lung Tissue Sampling: If the decision is made that a lung tissue sample (lung biopsy) is needed in order to make a diagnosis, there are a few different options:
Transbronchial Biopsy (TBBx) with Bronchoalveolar Lavage (BAL) can be done to obtain a very small piece of lung tissue and also a sample of a ‘washing’ of sterile water in and out of the lungs. It is performed as an outpatient procedure.
Blood Tests:
There are different types of blood tests that may be ordered to assist in making an accurate diagnosis Serology: These are blood tests that look for antibodies (proteins made by your immune system) in blood to determine if patient have a type of autoimmune disease (lupus, slceroderma, Sjögren's sydrome, polymyositis/ dermatomyositis, mixed connective tissue disease).
Examples of these blood tests include:
Rheumatoid Factor: rheumatoid arthritis
ESR: estimated sedimentation rate
CRP: C-reactive protein reflecting a response to inflammation
ANA: Antinuclear Antibodies
anti-dsDNA: anti-double stranded DNA
anti-SSA (Ro) and anti-SSB (La): anti Smith antigens
Anti-JO-1
ANCA: antineutrophil cytoplasmic antibodies
anti-Scl 70: scleroderma
5. How would you manage this condition?
Pharmacological Treatment to suppress further inflammation includes medications such as : Corticosteroids /Prednisolone , Azathioprine, Cyclophosphamide, Hydroxychloroquine and Methotrexate.
Anti-Fibrotic (anti-scarring) Agents include medications like Nintedanib (Ofev®) and Pirfenidone (Esbriet®, Pirfenex®, Pirespa®.
Non-pharmacological options include : Pulmonary Rehabilitation , oxygen and Palliative Treatment.
Pulmonary Rehabilitation (PR) is a structured exercise and education program for people with chronic lung diseases, including ILD, with the goal of maximizing a patient’s ability to maintain activity, decrease breathlessness and fatigue, and improve quality of life.
Typically, pulmonary rehabilitation will include exercise training (aerobic, strengthening, flexibility); breathing exercises; anxiety, stress, and emotional management strategies; nutritional counseling; disease education; medication education, and other components.


 https://drive.google.com/file/d/1M2Oi6_m0GhXR2KN7E43HcdwYCU59cIFQ/view?usp=sharing
https://drive.google.com/file/d/1M2Oi6_m0GhXR2KN7E43HcdwYCU59cIFQ/view?usp=sharing



Although simple, the CHADS2 score does not include many common stroke risk factors, and its limitations have been highlighted by its non-inclusion of common stroke risk factors. Even patients classified as low risk by CHADS2 in its original validation study have a stroke rate of 1.9% per year, which is close to the criterion of a cardiovascular event rate of 20% over 10 years for primary prevention strategies.
Consequently, CHADS2 was expanded to include three additional independent risk factors: vascular disease (coronary artery disease, peripheral artery disease, aortic atherosclerosis), age 65-74 years, and female sex.
This new, more inclusive scoring system is the CHA2DS2-VASc score.
The CHA2DS2-VASc score better discriminated stroke risk in nonvalvular AF subjects with a baseline CHADS2 score of 0 to 1
Table 3. CHA2DS2-VASc Score and Risk Criteria
Score | CHA2DS2-VASc Risk Criteria |
1 point | Congestive heart failure |
1 point | Hypertension |
2 points | Age ≥75 years |
1 point | Diabetes mellitus |
2 points | Stroke/Transient Ischemic Attack/Thromboembolic event |
1 point | Vascular disease (prior MI, PAD, or aortic plaque) |
1 point | Age 65 to 74 years |
1 point | Sex category (ie, female sex) |







The CHADS2 score (congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, stroke) was developed to more accurately predict the risk of stroke in patients with nonrheumatic AF.A score of 0 is classified as low risk. 1-2 is moderate risk , and more than or equal to 3 is classified as High risk.